


Billy, don’t be a fool with your life
If you are, blame someone else. Fags, HIV and narcotics.

HIV
It started with HIV. The first big disease that was all your own fault. Up until HIV and AIDS, disease was something that happened to you. Measles, smallpox, malaria, yellow fever: they were all transmitted in circumstances that couldn’t be helped. The poor patient was afflicted by these dreadful life-threatening diseases. Poor thing.
Even head lice or fleas were something that was only partly the sufferer’s fault. The main culpability lay with the dirty people who surrounded them. There was syphilis, of which Gustav Mahler, the Austrian composer, was so mortally afeared that he gained a reputation for frigidity, and even became one of the first ever to lie on Sigmund Freud’s couch in belle-époque Vienna. Gonorrhoea would become the young rake’s affliction, warranting nothing more than a dig with an elbow and a wink of the eye as moral reprimand. Almost a rite of passage, your first dose of the clap is. And more fool you if you get crabs into the bargain.
But HIV was a whole different kettle of fish. Writer John Doyle in his novel The Heart’s Invisible Furies describes a not entirely fictionalised encounter (edited here) between a straight man and his doctor telling him he has contracted the virus, told at a restaurant in New York from which the party is requested to leave, for their audacity of being gay in a public place:
“The fact is, until the heterosexual community accepts that this affects them too,” said Bastiaan putting his knife and fork down, “Nothing is ever going to get any better. There’s a patient in Mount Sinai at the moment. Patient 741. This guy had been getting terrible headaches for a few weeks and then he developed a cough that he couldn’t shake. He tried antibiotics but they hadn’t done any good. His local doctor ran some tests and she had her suspicions about what it might be so she sent him to me for a consultation. I knew when I saw him that she was right. I could tell just by looking at him but I didn’t want to alarm the poor guy unnecessarily by saying anything until I was absolutely certain, so of course I ran the usual tests.”
“How old is he?” asked Courtney
“Around our age; no wife, no children, but not gay. He had that sense of entitlement and arrogance that goes with really good-looking straight guys. He told me how he’d spent a lot of his life globetrotting and was worried that he’d picked up a bug along the way, malaria or something, and I asked him whether he was sexually active. Of course I am, he said, laughing as if the question was ridiculous I’ve been sexually active since I was a teenager. I asked him whether he’d had many partners and he shrugged and said that he lost count. A couple of hundred at least, he told me. Any men? I asked him, and he shook his head and looked at me as if I was crazy. Do I look like I have sex with men? he asked, and I didn’t bother answering him.
When he came back in for his results a week later I sat him down and told him that I was very sorry but that I’d identified the HIV virus in his bloodstream and although he had yet to develop full blown AIDS and we might be successful in warding it off for some time, there was a distinct probability that the virus would mutate into the full blown disease within a few months and of course as he probably knew there was no cure at the moment.
“So how did patient 741 take it?” asked Courtney.
“He didn’t take it well. He looked at me as if I was playing some crazy practical joke on him. Then he started shaking, visibly shaking, and asked me for some water. I went out to get some and when I came back he’d taken his file off my desk and was reading through it like a madman as if he wanted to prove to me that I was wrong. I took the file back and handed him his water but his hands were trembling so badly that he spilt it all over himself when he tried to drink it. When I finally calmed him down he told me that there was no way I could be right in my diagnosis and he wanted a second opinion. You can have one of course, I told him, but it’s not going to change anything. These are very specific tests in place today for how we identify the virus and there’s simply no doubt about it whatsoever. I am very sorry.
“But despite all this, patient 741 was still not willing to accept the truth. He wanted to know who the best doctor in the field was, where was the best hospital; he insisted that someone must be able to help him. That someone would be able to prove me wrong. But, doctor, he said leaning forward and taking me by the shoulders as if he wanted to shake some sense into me, I can’t possibly have that disease: do I look like a queer? I’m normal for Christ sake!”
“You see!” said Courtney, sitting back and throwing her hands in the air. “No education, no understanding at all!”
“In the end I had to call security: he started to lose his mind, came round to my side of the desk, pinned me up against the wall. He said he knew that I was a dirty faggot too and that I shouldn’t be allowed anywhere near patients, that I was probably infecting them one by one. Finally he backed off and that’s when he just crumbled and started to cry. Jesus Christ, he said, what will they say at home, what will they think of me?”
Yes, what would they think of him? What would they think of him for sowing wild oats in the course of his globetrotting? Oh, that? Perfectly normal. But, of course, it’s not normal to catch the gay plague. Tell me, what is it that makes a plague gay? Go and ask them that in southern Africa, where patriarchy and bravado, the inherent right of mankind to sleep around, at one point even brought us the Omicron variant of Covid-19.
I leave the reader to figure the real reason that makes a plague gay. But whether we’re talking HIV, diabetes, heart disease, obesity, the culprit is rarely the real culprit. Scapegoats abound in all our modern wars: against drugs, against heart disease; the war against money-laundering, the war against corruption, the war against war: the more we do to stop it, the more it thrives. Unless, that is, stopping it, whatever it is, means making more money than letting it thrive.
When I came out to my brother, one thing he said to me was that he would always be by my side, and that’s something he has never let me down on. But I had to smile inwardly when he admonished me, “Don’t go catching AIDS.” I wanted to reply, “No, sure I won’t. I’ll make sure that I don’t deliberately catch a fatal disease. Because that would be letting the side down.” It felt a bit like the song, Billy, Don’t Be a Hero. Except catching HIV is always your own fault. I mean, what is someone who gets infected by plasma to say? “I have HIV but, honest, I’m straight, y’see, got it from a dirty blood transfusion”?
So, HIV was really the first disease that’s all your own fault. Tsk, if only people didn’t have sex. Except those straight globetrotters, of course. They can have sex. They can even lose count. Worst that can happen is a case of the clap.
Cigarettes
Then came lung cancer, hot on HIV’s heels. Difference with lung cancer was that it was a universal disease, but identifiable victims. They had smoke coming out of the nose and mouth. They smelled of stale ashtrays. Hung around the entrances to office blocks. Sat upstairs on the bus. Or on the left-hand side of the cinema, back of the aircraft. Smokers. Had it coming to them. Could even infect non-smokers.
I think it’s pretty hard to decide which was the greater pariah: the smoker or the gay. Because even a smoker who doesn’t have cancer and doesn’t therefore cause all that cost to the health system, well they could get cancer, so it was almost as if they already did have it. I was at a meeting last summer in someone’s garden and this woman arrived late and sat down and there was some talk of smoking and she pulled out a packet of 20 and said, “Well, I’m bloody well going to smoke,” and I wondered whether it had even occurred to her to ask the other seven people present whether that was okay. But I know the answer: no. Thing is, the other seven were too polite to tell her to stuff her fags where the sun doesn’t shine. So, there’s still a bit of friction between smokers and non-smokers, both of whom recognise, now at least, that both of them can get lung cancer, sometimes from the same cigarette. I felt like asking the lady, purely out of politeness, you know, whether she minded me having a bit of unprotected penetrative sex whilst they talked, but there was no one there I fancied, so I kept stumm, like all the rest.
Now, there are oodles of diseases that are all your own fault: heart disease, diabetes, obesity, but people mostly have great sympathy for sufferers because, like when everyone was smoking, there’s a kind of acceptance of the fact that, if we stuff our faces with sugar, processed grains and canola oil, then everyone is as susceptible to heart disease and diabetes as we used to be to malaria and smallpox. In Africa, that is.
Who is to blame for what diseases therefore knows a great deal of variance across societies, across countries and across the world. Malaria is caused by a mosquito. If you’re inoculated against it, it does no harm. But if you’re one of the millions in Africa who are not inoculated, you can die of it. Inoculating the entire continent of Africa would in fact cost very little. But it’s never been done, so people continue to die of malaria in Africa, and other tropical regions of the world. We in the west don’t see the problem as an immediate danger. It might not be their fault, but it’s not our responsibility. Because we say so.
Flying is the safest mode of transport in the world, statistically. But, on an aeroplane the potential for something to go amiss is much greater than when crossing the street. And yet people get killed crossing the street much more than in air accidents. Because the potential for a mishap is covered by the extra care taken when operating an aeroplane. Deaths on the street come because people are careless, both when walking and when driving. And far more people cross streets than fly in aeroplanes, so the chances are that bit greater.
The potential danger of crossing the road is more generally realised because of a lack of perception that it even exists. For example, I pay great attention now to silent vehicles like electric cars and bicycles. I watch out for what I cannot hear, after a lifetime of being used to listening as well as looking to cross the road. I perceive the danger. But one day I might not. Then I’ll get killed. And no one will attribute my death to a bicycle whizzing down my 30 kph-limit street at 45 kph. They’ll attribute it to me. Because it’s to me that people want to attribute it.
The trick with cigarettes is not to inhale. Just like Bill Clinton said.
Drugs
The danger of drugs is addiction, they say. If you take drugs, like smoking, then you can develop a dependency on them. You always need to have more. Even of the ones that render you listless and dozy. But not the ones that kill you—you never need more of those. As long as drugs don’t kill you, and you have the cash to sustain your habit, many people think that they’re able to continue indulging it. They have the habit under control.
I’m unable to judge whether anyone in particular has their habit under control or not, and I have understanding for those who like to pop an ecstasy in order to party the night away at a rave. Raves where everyone is on ecstasy are the politest crowds of people you’ll ever encounter: “Oh, I’m terribly sorry, did I spill some beer on your feet?” “No problem, dear chap, they’re an old pair of shoes anyway! Would you care to dance?” That sort of exchange (except in straight discos, where there’s more of an ambience of machismo …).
Addiction and antisocial behaviour are the very thick end of the drugs wedge. So thick that, with a little bit of will and a little bit of self-control, it can in fact be grabbed and held to account. Because when most individuals come down from their drug-induced high, many of them do, when all’s said and done, return to their senses. They may even have misgivings about things they said or did whilst under the influence. They may even have done things that are uncharacteristic of them, and recognise that fact. But, no matter: a new week begins, and next Friday is another day.
The thick end of the drugs wedge is not really a major issue. It is the thin end that’s of greater concern. The thin end is where drug use starts to influence policy.
Among young people, drug abuse is in fact reducing. I won’t say it’s on the wane, but gen Z is actually starting to show the way in terms of both alcohol and drug use.
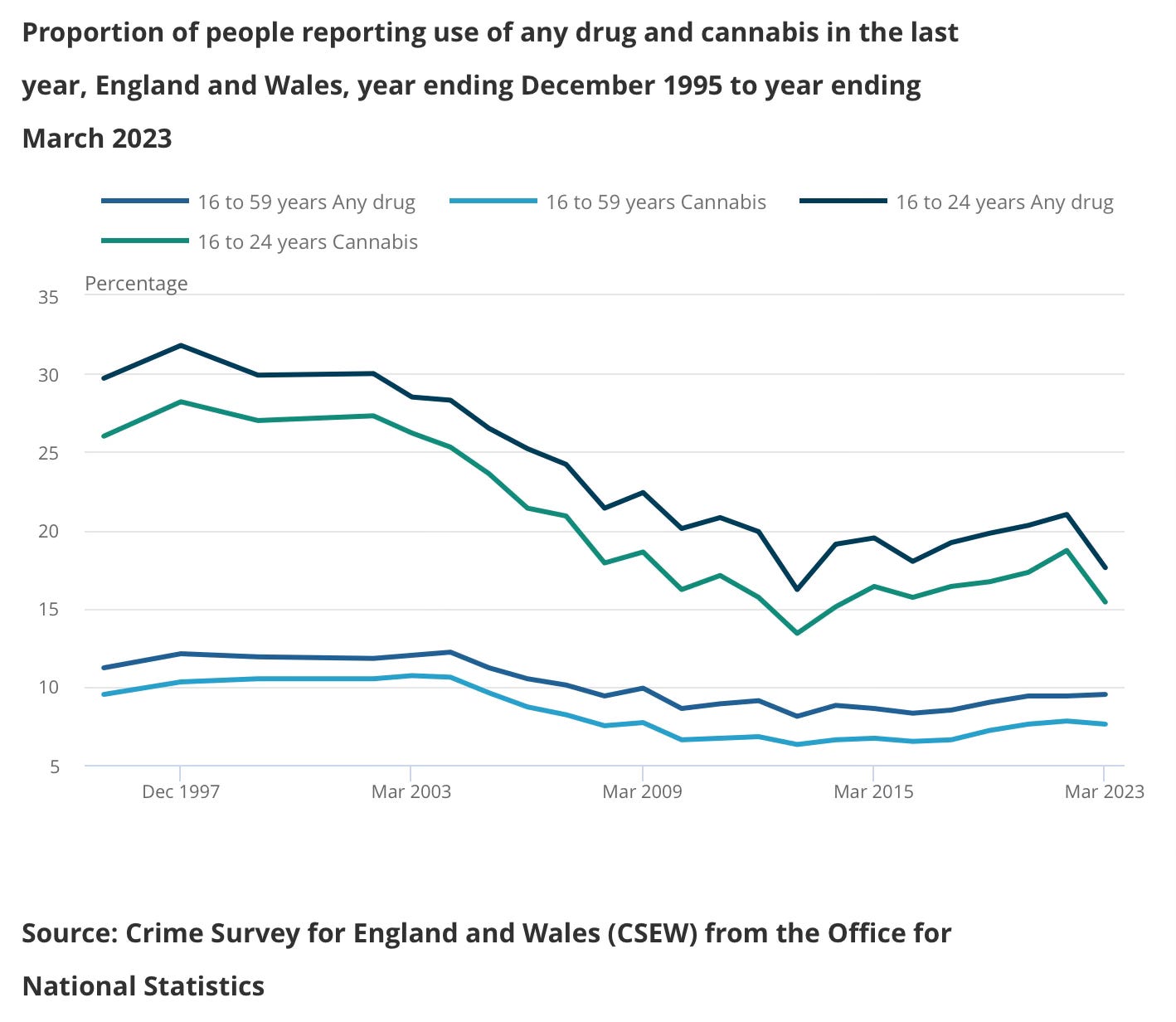
Of course, there could be a reporting gap but it’s to be assumed that the methods for collecting this data remain constant, so that a trend is a trend, even if concrete figures may be misleading. However, around the world, and drugs are a worldwide issue, consumption is very much on the up, far more widespread than it was even at the turn of the millennium. And part of the reason for that is that those in power are far more susceptible to the pressures applied by drug barons and are far more amenable to their demands in terms of policy.
[W]e have allowed the criminal cartels to eat western democracies from the inside.
What is happening in Ecuador is a story that concerns everyone, because drug use is not an exception now but the norm. Last year, an international study found that British people have become the second-biggest cocaine users in the world. And it is not just a moral issue, because drug trafficking and mafias mean doped markets, businesses with unfair competition, corruption and manipulation of public consensus, and, ultimately, the destruction of democratic rules of government.
The world is hungry for cocaine and happy to buy it. But think of the ravaged countries that pay the price by Roberto Saviano
The concerns now arising, therefore, are not those surrounding addiction in and of itself. It’s that its controllability is slipping away from users’ grasp, from that thick end to the thin end of the wedge. With time and, above all, with the workaday nature of drug-taking, with use moving across societies to the point that it’s no longer a moral issue to be taking stuff, it’s the social acceptability of hard drugs that is now the impending threat. The weekend partiers are no longer just social drop-outs, pop singers and hallucinating college kids; it’s your bank manager, it’s cops, it’s politicians, it’s middle-class executives, it’s anyone and everyone. And, as drugs start to permeate society, as their acceptability means revelations get met more with a sniff (pardon the pun) than wide-eyed consternation, users start to have widespread effects on the general tenor of society, the judgments that get made, the bloody-mindedness with which policy is pursued, whether at board room, at governmental, or patriarchal level.
The money flows are breathtaking. Dirty money that streams across the globe like some atmospheric river, falling not as raindrops but as dollar bills. Onto the Caribbean’s tax havens they fall (or not, a factor contributing to yet other central American problems, such as Haiti’s and Venezuela’s). With rapacious appetites for drugs across the western world, the very problem that consumers create in the first place is used as a policy tool to repel those labelled as the problem’s cause: the women and children drowning in the Rio Grande on Texas’s border to Mexico, the women and children being raped as they pass up the Darien Peninsula. Rural Americans lie doped to the eyeballs with narcotics that, once the stupor has worn off, they blame innocent immigrants of sneaking into their land of innocence, pure as the driven … snow.
“They bring naught but crime into the US.” “They freeload.” “They’re only here to profiteer.” It is true that MS-13 and its likes thrive on an influx of disenchanted, criminally minded migrants from the poorest reaches of central and south America. It is true that, if Venezuela’s oil income were duly and properly administered, Venezuela’s problems would not be inducing it to seek solace in a war with Guyana. And it is true that Sweden has seen a vicious uptick in criminal gang behaviour since it opened wide its arms to migrants from across Europe and the Middle East. But the question is: why?
Sweden’s migrant and gang issues may stem from the country being targeted by supposed refugees as a nest from which to expand their criminal operations but, if I were aiming to establish a criminal network 15 years ago, I’m not sure that Sweden would’ve been my first choice. Now, perhaps, things are different. And, quite honestly, the problem of criminality is an issue that has lain unattended-to for too long in Sweden. The chief commissioner of Stockholm’s police was warning of the impending sea change 20 years ago, and her warnings were not heeded. Sweden’s migrant problem is due to Sweden’s insouciance to matters of integration, employment, education and, bluntly, listening to the cops who in fact know best.
Much of the gang activity, whether in Sweden or elsewhere, is fed by a hunger for narcotics. That is no less the case in Europe than in North America. Stop consuming drugs and you will stop the vast majority of gang activity. Those who slip a quick 8-ball think they’re doing no one any harm: but they are sustaining the whole filthy business. Few addicts hold more than an eighth of an ounce at any one time. So everyone’s ultimate consumption will be small potatoes. Everyone who’s shooting up a 0.1 slam thinks What possible harm can this be doing? (aside, that is, from turning their brains to cheese).
It is not the slam, and it’s not the 8-ball. It’s that, five times in every street, fifty times in every district, a thousand times in every town, ten thousand times in every county, 100,000 times in every state, every day of every year, across a nation, across the world. Not just down-and-outs, but lawyers, doctors, steelworkers, shopkeepers, lorry drivers, taxi cab drivers, pile drivers. If middle-class workers would stem their desire for illicit product, the gangs would wane. If the drug barons cannot be reined in, then part, at least, of the reason lies in government not really wanting to.
There are no end of takes on drugs. We could treat them as pharmaceuticals and allow them only on a doctor’s prescription. However, as the scandal in the hospice sector in the US shows, and in the medical approval of insurance claims, and scandals in gynaecology at Columbia University, etc., etc., etc., it’s clear that doctors are as inclined to sign off on whatever gets them a kick-back (or a kick) as anyone else.
We could treat drugs like tobacco: legalise them, restrict sales, monitor quality and take a margin for the government in terms of turnover tax. Make the government into a drug dealer. Whatever next?
We could clamp down like crazy on drug imports. In fact, if government were halfway serious about attacking the drug problem, they would have done this decades ago. So why don’t they? They know when you pick your nose in the street, and they can’t detect drugs being flown or shipped in by the bucketload? There is a temptation to say that the government is already a drug dealer. Because when you don’t pick up even a small percentage of the illegally imported product, either your homeland security sucks or it’s because you don’t want to.
The only way to stem the flow that would work guaranteed is to stop using it. If there is no market, the gangs will move on to something else. Like canola oil. The Italian Mafia has already moved away from drugs: they’re bulky, they’re smelly, the distribution channels are too unreliable. So, the Mafia is now into olive oil, tomatoes, pasta. They can flog those through legit channels and set up ghost channels that claim billions in subsidy from the EU. Are there no olives and tomatoes in Mexico?
The main source isn’t Mexico anyway. It’s China. China is wreaking its revenge for the Opium Wars, and there’s a part of me says, I don’t blame them. What was sauce for their goose is now sauce for our gander. And the Chinese know from bitter experience just how drug addiction can render an entire nation susceptible to easy influence. Because the West taught them.
If use doesn’t stop, then the next step is more or less much of the West becoming narco-states. If they aren’t already, that is.
Bravo, Graham, for writing about topics that are frequently swept under the rug. First on the malaria problem in Africa and the Mediterranean area: The reason many persons native to Africa have not been vaccinated has more to do with lack of education, long held religious beliefs, and lack of knowledge than insufficient vaccines. Colonialism did no favors to the Continent. Europeans came, and Europeans took, they did not give. Those African tribes that survived continued in their age-old beliefs. Oh, the Europeans brought new religion - whoop-de doo! That didn't stop the tribal religions and their reliance on questionable practices. One of my dear friends is from Sierra Leone and he explained the rapid spread of the Ebola virus in the interior parts of Sierra Leone, apparently there is an age-old ritual that when a tribal member dies, the women wash the corpse and drink the water from the washing to ease the passing. It is these age-old beliefs, that must be overcome. Giving people a "new god" to worship may make the missionary feel vindicated, but it does little for the good of Africans.
On AIDS, I am truly sorry for the way gay men especially were mistreated. The utter stupidity of the 'straight' community is and always has been a blight. HIV is not easy to get, it is not airborne, it can only be transmitted by body fluid to body fluid. As you are aware, the use of condoms, ended the widespread infections among gay men. AIDS is more frequently transmitted now by sharing drug needles from what I have read. My daughter, Laura, as part of her pre-med program did an in depth research in HIV. Since I have a Masters in physiology she shared a lot of her findings and the final paper with me, the Human Immunodeficiency Virus mutates four to seven times in any 24 hours, therefor it took years to find pharmaceutical cures and vaccines. And any Homo sapiens is susceptible. Arthur Ashe, the tennis great, was infected by receiving a blood transfusion.
On cigarettes, I'm not so forgiving. When I was a youngster I smoked heavily for 8 years, 3 packs a day, unfiltered cigarettes. Really stupid, and no excuse. I cheated by getting pregnant and morning sickness broke my smoking habit, but I never again took up the habit. The problem now is I am highly allergic to cigarette smoke, it causes me to cough uncontrollably. Cigarette smoke is hard for non-smokers to avoid, as animals we have to breathe. If a smoker wants to have early onset heart disease, that is their choice, but they have no right to inflict their habit on other people. Smoking in public forces others to breathe in the smoke, it is unavoidable.
Finally, on widespread chemical (drug) usage, we do need to find some good way to mitigate it. Right now in America it is fentanyl that is killing young people, a few years ago the main culprit was opioids being foisted on the drug using population by the pharmaceutical industry - who in America are far more interested in increasing their wealth than in curing or preventing disease. There is also the role of mental health in using chemicals that are harmful to the body. When I was a science teacher I was asked to teach classes on avoiding physical damage to the human body. I prefer the term chemical dependency to drug abuse. Drugs are chemicals, you cannot abuse them, you can burn them, combine them with other compounds and since they are inanimate they don't care.